Zotec is always at the forefront of the radiology specialty, especially when it comes to CPT changes. Here we provide descriptions of the new and revised CPT codes impacting Radiology in 2023.
It’s important to note more detailed CPT instructions from various medical societies, ACR or SIR, have yet to be published. Also, the NCCI (National Correct Coding Initiative) policy manual has not yet been published. Zotec will provide more information to the radiology community as these publications are released.
New and Revised CPT Code Descriptions for 2023 are listed in the following categories:
Diagnostic Radiology
Nerve Ultrasound
SPECT Services
Interventional Radiology
Percutaneous Arteriovenous (AV) Fistula Creation
Somatic Nerve Injection
Paravertebral Spinal Nerve Injection
Percutaneous Nephrolithotomy
Category III Codes
CT Tissue Characterization
Quantitative MRCP
Biomechanical CT with Vertebral Fracture Assessment
Digital X-ray Radiogrammetry (DXR-BMD) for Bone Density Assessment
Evaluation and Management
AI Taxonomy Appendix
Diagnostic Radiology
Nerve Ultrasound
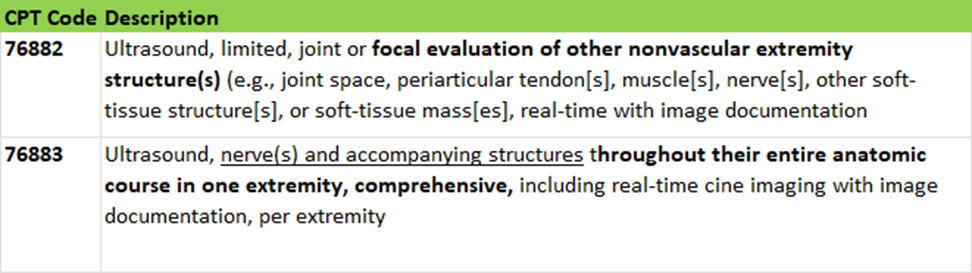
A new code has been created to report a comprehensive ultrasound of nerves and accompanying structures.
The descriptor for existing code 76882 (US joint or other nonvascular extremity structures) has been revised to include the phrase “focal evaluation of” other nonvascular extremity structure(s) to differentiate between a comprehensive study of a nerve(s) throughout its entire course versus a limited or focal evaluation of the nerve.
76883 requires evaluation of the entire course of the nerve in the extremity
76882 should be used for a focal evaluation of a nerve visualizing only one or two points in the extremity or anything less than the entire course of the nerve
SPECT Services
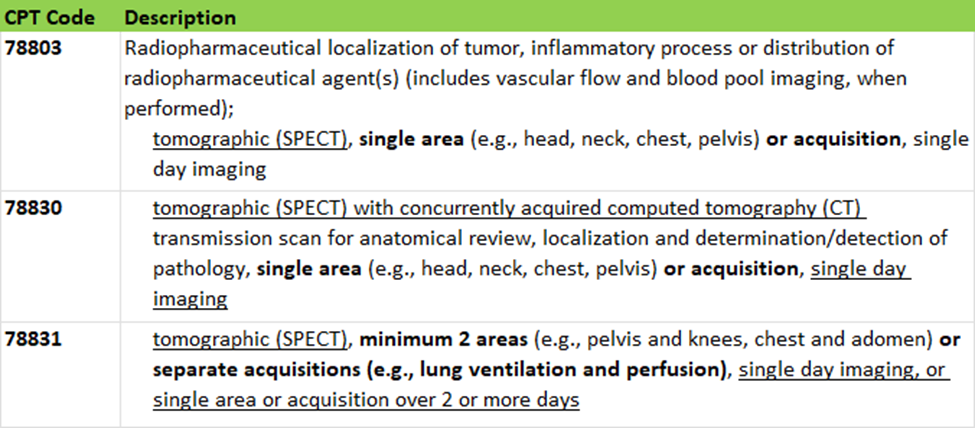
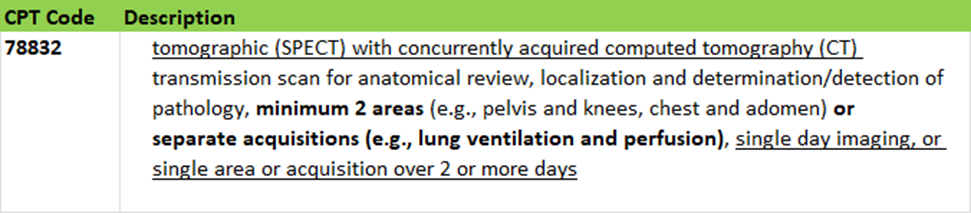
An editorial revision has been made to codes 78803 and 78830-78832 to clarify the intention of this family of codes and to differentiate
Single area or single acquisition examinations versus
Two or more separate acquisitions with two different radiopharmaceuticals on the same date of service or over two or more days
The intent and use of these codes remain the same
The term acquisition for the purpose of these codes is defined as “separately obtained imaging with different radiopharmaceuticals” even if they were obtained on the same day and from the same anatomic site.
Adding separate acquisition and the example of lung ventilation and perfusion allows for the intended use of these codes to include situations where multiple acquisitions of the same area are imaged as well as when multiple areas are imaged.
Interventional Radiology
Percutaneous Arteriovenous (AV) Fistula Creation
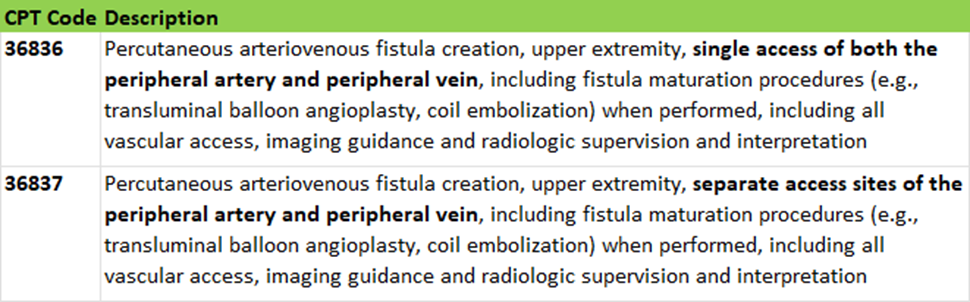
Two new codes have been created for percutaneous arteriovenous fistula creation. Previously there were only codes available for AV fistula creation via an open approach.
These codes are for upper extremity only.
If performed on the lower extremity, an unlisted code must be reported.
These codes include all vascular access, angiography, imaging guidance, and blood flow redirection or maturation techniques (e.g., transluminal balloon angioplasty, coil embolization) performed for fistula creation.
These services cannot be reported separately when performed at the same operative session.
36836 – Single-Access System (e.g., Ellipsys™)
Access via a single percutaneous puncture into an arm vein
A catheter is passed through the vein wall into the proximal radial artery (AV fistula)
Guided by Duplex US – no fluoroscopy
Produces a connection between the artery and vein via thermal energy
36837 – Two-Access System (e.g., WavelinQ-4F™)
An arterial catheter is introduced through the brachial artery
A venous catheter (with a radiofrequency [RF] electrode) is introduced through an upper extremity vein
Guided by fluoroscopy
Magnets are used to hold the artery and vein together
The RF electrode is then used to create a connection between the artery and the vein (AV fistula)
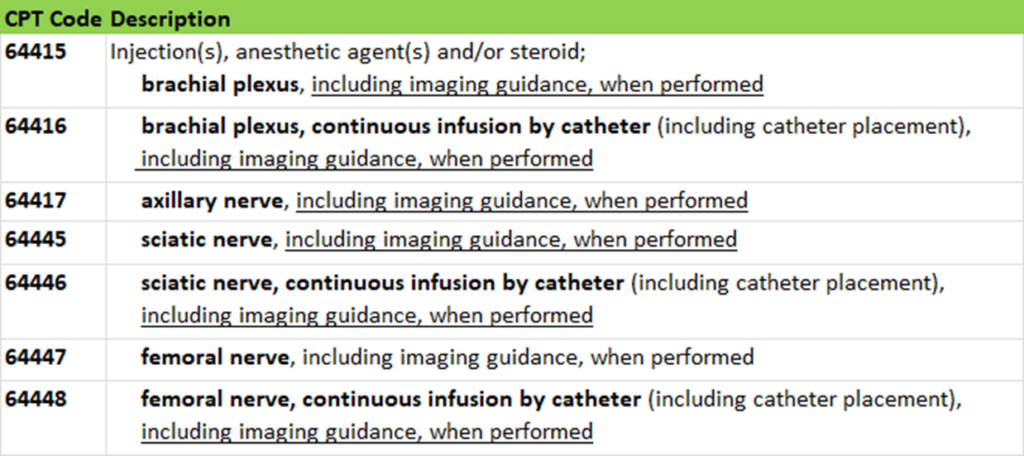
Somatic Nerve Injection
The somatic nerve injection codes (64415-64417 and 64445-64448) have been revised to include imaging guidance when performed.
CPT codes for imaging guidance (US – 76942, fluoro – 77002, 77003) can no longer be reported in addition to the somatic nerve injection codes.
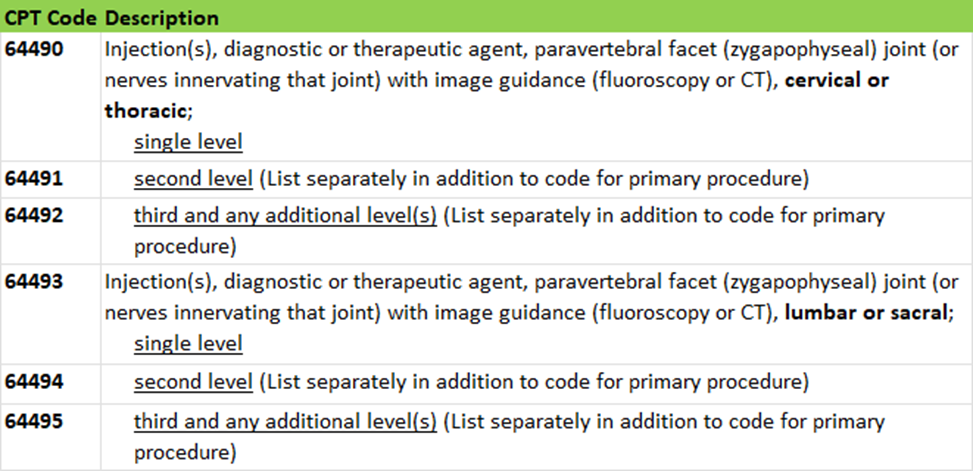
Paravertebral Spinal Nerve Injection
Several changes have been made to the Paravertebral Spinal Nerves and Branches Subsection of CPT to clarify the proper use of the codes. No changes were made to the code descriptions themselves.
The new instructions include:
Fluoroscopic or CT imaging guidance is required for paravertebral facet joint injections described by codes 64490-64495.
If imaging is not used, report 20552 or 20553 (trigger point injections).
If US guidance is used, report Category III codes 0213T-0218T.
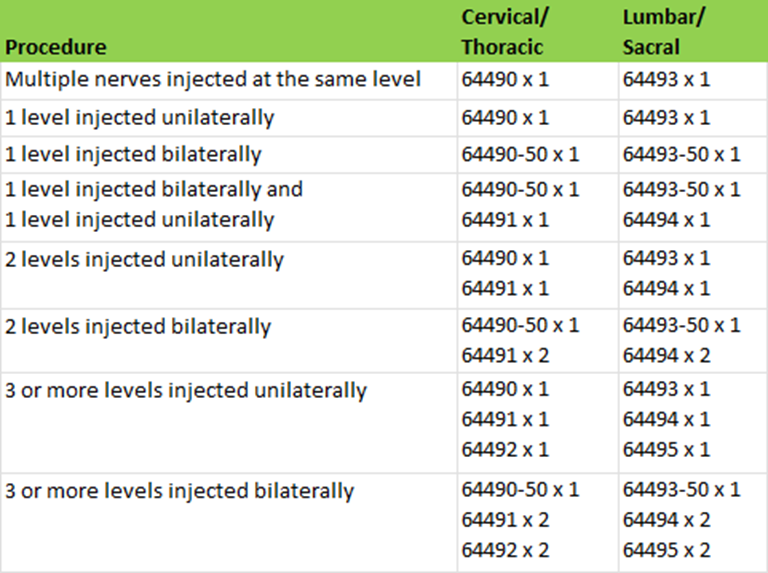
In order to determine a level, count the number of facet joints injected, not the number of nerves injected.
If multiple nerves of the same facet joint are injected, it is considered a single level.
The add-on codes (64491-64492, 64494-64495) are reported when second, third, or additional levels are injected during the same session.
When the procedure is performed bilaterally at the same level, report one unit of the primary code with modifier 50.
When the procedure is performed on the left side at one level and on the right side at a different level in the same region, report one unit of the primary procedure and one unit of the add-on code.
When the procedure is performed bilaterally at one level and unilaterally at a different level(s), report one unit of the primary procedure for each level and append modifier 50 for the bilateral procedure.
If the procedure is performed unilaterally at different levels, report one unit of the primary procedure and the appropriate add-on code(s).
For unilateral paravertebral facet injection of the T12-L1 and L1-L2 levels or nerves innervating that joint, use 64490 and 64494 once.
For bilateral paravertebral facet injection of the T12-L1 and L1-L2 levels or nerves innervating that joint, use 64490 with modifier 50 once and 64494 twice.
The following chart was added to CPT to aide in the understanding of the above instructions.
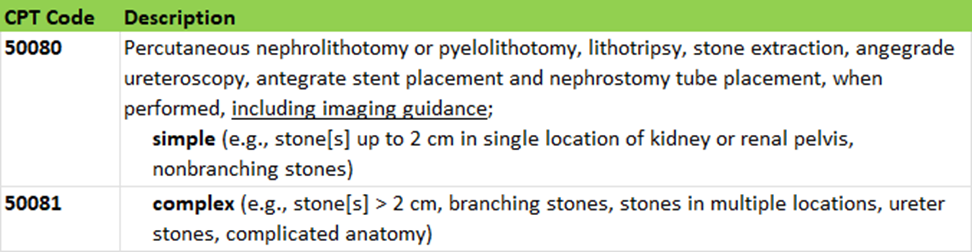
Percutaneous Nephrolithotomy
Revisions have been made to the following codes. New introductory guidelines and parenthetical notes have been added to provide clarity in reporting these services. The code descriptions have been updated to remove outdated terminology that is no longer used in current clinical practice.
Includes the antegrade removal of stones in the calyces, renal pelvis, and/or ureter with the antegrade placement of catheters, stents, and tubes
Does not include retrograde placement of catheters, stents, and tubes
Report 1 unit of 50080 or 50081 per side (i.e., per kidney), regardless of the number of stones broken and/or removed or locations of the stones
For bilateral procedure, report 50080, 50081 with modifier 50
When 50080 is performed on one side and 50081 is performed on the contralateral side, modifier 50 is not applicable
Placement of additional accesses, if needed, into the kidney, and removal of stones through other approaches (e.g., open or retrograde) may be reported separately, if performed
Category III
These are a set of temporary codes for emerging technology, services, procedures, and service paradigms. Category III codes allow data collection for these services/procedures. If a Category III code is available, this code must be reported instead of a Category I unlisted code. The use of the codes in this section allows physicians and other qualified health care professionals, insurers, health services researchers, and health policy experts to identify emerging technology, services, procedures, and service paradigms for clinical efficacy, utilization, and outcomes. A service/procedure assigned a Category III code does not guarantee recognition or reimbursement from third party payers.
The following codes relevant to radiology were effective July 1, 2022. These codes were added to the CPT manual with the 2023 edition. (See the AMA website for a full list of Cat III codes effective in 2022 and 2023)
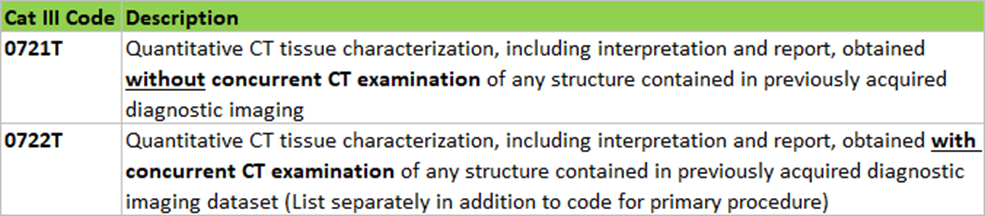
CT Tissue Characterization
Quantitative CT tissue characterization is a new technology that can improve population health strategies and lead to better patient outcomes by using computer algorithms to quantitatively characterize tissues on CT images that could only be subjectively evaluated in the past.
Report 0721T for Quantitative CT tissue characterization performed retrospectively on a previously acquired CT scan
Report 0722T when Quantitative CT tissue characterization is performed with a concurrently obtained CT scan
Report 0722T in addition to the appropriate CT code
Quantitative MRCP (QMRCP) is the quantitative evaluation of pancreato-biliary structure anatomy from MR images that produces quantitative data of the biliary tree and pancreatic ducts. The data can inform radiologist evaluation and interpretation, aid physician decision making, and potentially reduce the time for initiation of targeted treatments and interventions in diseases, such as cholestatic liver disease, chronic pancreatitis, or gallstones.
Report 0723T for QMRCP performed retrospectively on a previously acquired MR scan
Report 0724T when QMRCP is performed with a concurrently obtained MR scan
Report 0724T in addition to the appropriate MRI abdomen code (74181-74183)
3D post-processing cannot be reported in conjunction with 0724T
The following codes relevant to radiology are effective January 1, 2023.
Biomechanical CT with Vertebral Fracture Assessment
This new category III code has been established to report bone strength and fracture risk assessment using finite element analysis of functional data and bone mineral density with concurrent vertebral fracture assessment.
The difference between new code 0743T and the existing codes 0554T-0557T is that the new code includes vertebral fracture assessment.
Code 0743T can be reported either by itself when performed on an existing CT dataset or can be reported in conjunction with code 0558T when performed with a concurrently obtained CT scan taken for the sole purpose of performing biomechanical CT analysis.
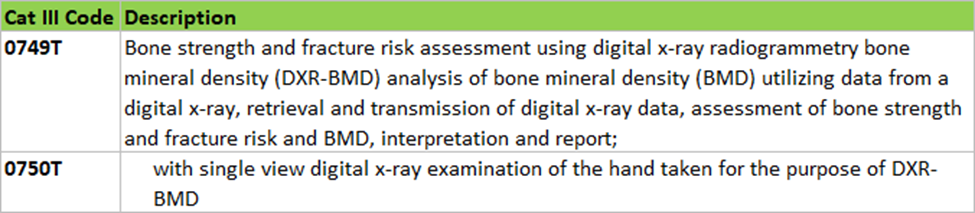
Digital X-ray Radiogrammetry (DXR-BMD) for Bone Density Assessment
Two Category III codes have been created for reporting bone strength and fracture risk assessment using digital x-ray radiogrammetry bone mineral density (DXR-BMD) analysis.
Code 0749T is reported for DXR-BMD analysis of an available appropriate digital x-ray (e.g., hand/wrist).
0749T should be reported in addition to the appropriate x-ray code.
Code 0750T is reported when an appropriate digital x-ray is not available, and a single digital x-ray view of the hand is taken specifically to be used for DXR-BMD analysis.
Evaluation and Management
The most highly anticipated changes are in relation to E/M for non-office/outpatient services (office/outpatient services were revised in 2021).
The E/M changes to the office/outpatient codes from 2021 and the new changes to other non-office/outpatient codes effective for 2023 were made with the following guided principals in mind:
Decrease administrative burden of documentation and coding
align CPT and CMS whenever possible
Decrease the need for audits
Decrease unnecessary documentation in the medical record that is not needed for patient care
Ensure that payment for E/M is resource-based and that there is no direct goal for payment redistribution between specialties
Highlights of major changes include:
Removal of documentation requirements for History and Exam for the purpose of code selection
Document what is necessary for patient care
Medical Decision Making (MDM) or time are the only determinants of code level
Time based billing
Number of minutes required for each code has changed
Total time on date of encounter can be counted
Counseling and coordination of care time is no longer a factor
Observation codes have been deleted
Inpatient codes now include observation services as well
Place of Service distinction will still exist
Inpatient and Observation Care Services
Revision to guidelines
Revision of codes 99221-99223, 99231-99236, 99238-99239 to include observation care services
Deletion of codes 99217-99220 and 99224-99226
Consultations
Revision to guidelines
Revision of codes 99242-99245 and 99252-99255
Deletion of codes 99241 and 99251
Emergency Department Services
Revision to guidelines
Revision of codes 99281-99285
Nursing Facility Services
Revision of codes 99304-99310
Deletion of code 99318
Home and Residence Services
Revision to guidelines
Revision of codes 99341, 99342, 99344, 99345, and 99347-99350
Deletion of codes 99324-99328, 99334-99337, 99339, 99340, and 99343
Prolonged Services
Revision to guidelines
Creation of 99418 for prolonged services in the inpatient and observation setting
CMS created its own set of HCPCS codes to be used to report prolonged services based on different timeframes than CPT (G0316, G0317, G0318)
Revision of codes 99417 and 99483
Deletion of codes 99345 and 99355-99357
New Artificial Intelligence (AI) Taxonomy Appendix
Appendix S was newly added to CPT for the 2023 edition to report Artificial Intelligence Taxonomy for Medical Services and Procedures.
The AI Taxonomy provides and defines distinct categories to describe the work done by the machine on behalf of the physician based on:
Technical features and performance of emerging AI products and services
Effect on the work of the physician or other QHP
Discrete components of work in order to facilitate valuation
Goals of the AI Taxonomy
Establish foundational definitions
Define elements of differentiation
Be understood by stakeholders who are not AI experts
AI has been classified into one of these three categories:
Assistive – The machine detects clinically relevant data without analysis or generated conclusions
Requires physician or other QHP interpretation and report
Augmentative – The machine analyzes and/or quantifies data in a clinically meaningful way.
Requires physician or other QHP interpretation and report
Autonomous – The machine automatically interprets data and independently generates clinically meaningful conclusions without concurrent physician or other QHP involvement.
Includes interrogation and analysis of data
The clinically meaningful conclusion may be a characterization of data to be used to establish a diagnosis or to implement a therapeutic intervention
There are three levels with varying physician or other QHP professional involvement:
Level I – Draws conclusions and offers diagnosis and/or management options, which are contestable and require physician or other QHP actionto implement
Level II – Draw conclusions and initiates diagnosis and/or management options with alert/opportunity for override, which may require physician or other QHP action to implement
Level III – Draw conclusions and initiates management, which require physician or other QHP action to contest