In December, CPT Assistant published new authoritative guidance for the coding of pain blocks. Previously there has been some confusion on when to assign 64450 (Injection(s), anesthetic agent(s) and/or steroid; other peripheral nerve or branch) or 64999 (Unlisted procedure, nervous system). This article clarifies how nerve blocks versus fascial plane blocks are to be reported. To illustrate the differences, a section of the guidance is referenced below.
CPT codes that describe perineural blocks, such as femoral nerve blocks, cannot be used to report procedures that target fascial planes where the work performed is distinctly different. There are key differences in the work performed for planar blocks. Existing CPT codes for neural blocks (64400 – 64485) identify a specific nerve or nerve branch, as opposed to fascial planes, which are innervated with sympathetic and nociceptive fibers. Local anesthetic injected into a fascial plane may act on both sympathetic and somatic nerves and branches traversing through the fascial plane. In addition, the fascial course of nerves is highly variable. How far they travel within the plane and enter and exit the plane is inconsistent.
In addition, most planar blocks target the deep fascia. There are two types of fascia: epimysial and aponeurotic fascia. Epimysial fascia, for example, as found in the pectoral region, is thinner and more adherent to the muscles (relevant to the PECS II block). Aponeurotic fascia is thicker, easily separated from the muscle and is seen in the thoracolumbar fascia (TLF), which is the target for the erector spinae plane (ESP) and quadratus lumborum (QL) blocks.
Because of the difference in the work performed, CPT codes for perineural blocks, such as femoral nerve blocks, cannot be used for procedures that target fascial planes where the work performed is distinctly different. The work involved in performing a fascial plane block is different from the work required to perform a perineural block, even though multiple nerves and branches may well be present in the fascial plane.
For fascial plane blocks that do not have a specific CPT code and in which the injectate is deposited into a fascial plan (as opposed to a perineural to a specific nerve), code 64999, Unlisted procedure, nervous system, should be reported. When blocks that deposit injectate perineural for a specific peripheral nerve or branch are performed and that do not have a designated CPT code, code 64450, injection(s), anesthetic agent(s) and/or steroid; other peripheral nerve or branch, may be reported.
This new guidance has resulted in an ever-growing number of blocks that we now report with the unlisted CPT code 64999.
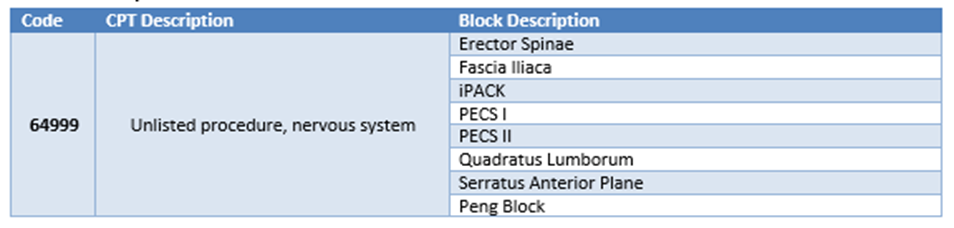
In summary, facial plane blocks that do not have their own CPT code are now required to be reported with unlisted CPT code 64999. Other peripheral nerve blocks (such as radial, ulnar, common fibular, peroneal, etc.) are to be reported with 64450 (Injection(s), anesthetic agent(s) and/or steroid; other peripheral nerve or branch). The challenge in reporting unlisted CPT codes, is that these codes do not carry RVUs or set fees; therefore, reimbursement is left up to the payers’ discretion. The fact that each block presents its own unique set of necessary skill and risk which can change the expected reimbursement from one procedure to the next adds to the complexity for the expected reimbursement of these types of procedures.
By: Pamela Linton, CPC, CANPC, Manager, Corporate Coding
Learn more about Zotec Partners here.



